| Key Takeaways Ovulation induction uses medications to stimulate egg development in women who don’t ovulate regularly.Clomiphene citrate and letrozole are the most common oral medications used, costing INR 200-600 per cycle.Injectable gonadotropins are used when oral medications fail, costing INR 5,000-20,000 per cycle.Follicle monitoring scans every 2-3 days track development and confirm ovulation timing.According to ICMR, ovulation induction is the first-line treatment for anovulatory infertility.PCOS affects 10-15% of Indian women and is the leading cause of ovulation problems requiring induction.Success rates per cycle with ovulation induction alone are 10-20%, rising to 15-25% when combined with IUI. |
| Quick Facts Clomiphene citrate cost per cycle: INR 200 to INR 600 Letrozole cost per cycle: INR 300 to INR 800 Gonadotropin injections per cycle: INR 5,000 to INR 20,000 Monitoring scan cost per scan: INR 800 to INR 2,000 HCG trigger injection: INR 500 to INR 1,500 Success rate per cycle (OI alone): 10-20% |
Ovulation Induction in Pune: Statistics 2025-2026
| Metric | Data Point | Source |
| PCOS prevalence in Indian women | 10-15% | ICMR 2024 |
| Anovulation as infertility cause | 25-30% of female infertility cases | WHO 2022 |
| Ovulation induction success per cycle | 10-20% | ICMR 2024 |
| OI + IUI combined success per cycle | 15-25% | PubMed 2023 |
| Clomiphene ovulation rate | 70-80% of women treated | Industry estimate |
| Letrozole success in PCOS vs clomiphene | Superior per multiple studies | PubMed 2022 |
| OHSS risk with gonadotropins | 1-5% moderate or severe | ICMR 2024 |
What Is Ovulation Induction?
Ovulation induction is the use of medications to stimulate the development and release of one or more eggs in a woman whose ovaries are not producing eggs on their own. The goal is to create the conditions for natural conception or to time egg release precisely for IUI.
Women who benefit most are those with irregular or absent periods due to PCOS, hypothalamic amenorrhoea or unexplained anovulation. The treatment is also used in regularly ovulating women to produce 2-3 follicles simultaneously, increasing the chances of conception per cycle when combined with IUI.
Is ovulation induction the same as IVF? No. Ovulation induction stimulates the ovaries to release eggs naturally, and fertilisation happens in the body. IVF retrieves eggs from the ovaries and fertilises them outside the body in a laboratory. Ovulation induction is a much simpler, less expensive process.
Medications Used for Ovulation Induction in Pune
| Medication | Type | Dose | Cost Per Cycle (INR) | Best For |
| Clomiphene citrate | Oral tablet | 50-150mg Day 2-6 | 200 to 600 | Unexplained infertility, mild PCOS |
| Letrozole (Femara) | Oral tablet | 2.5-7.5mg Day 2-6 | 300 to 800 | PCOS (now preferred over clomiphene) |
| Gonadotropins (FSH/hMG) | Injectable | 37.5-150 IU daily | 5,000 to 20,000 | Failed oral agents, low AMH |
| HCG trigger injection | Injectable | 5000-10000 IU once | 500 to 1,500 | All OI cycles to time ovulation |
| Progesterone luteal support | Vaginal/oral | Post-ovulation | 1,000 to 2,000 | After IUI or timed intercourse |
Letrozole vs Clomiphene for PCOS: Why the Recommendation Has Changed
For years, clomiphene citrate was the standard first-line medication for ovulation induction in women with PCOS. Multiple well-conducted trials, including the landmark PPCOS II trial published in the New England Journal of Medicine, showed that letrozole produces higher live birth rates than clomiphene in women with PCOS.
Letrozole works by temporarily reducing oestrogen levels, which causes the pituitary gland to increase FSH and stimulate follicle development. Unlike clomiphene, letrozole doesn’t affect the endometrial lining adversely and has fewer anti-oestrogenic side effects. ICMR 2024 guidelines now recommend letrozole as the preferred first-line agent for ovulation induction in PCOS.
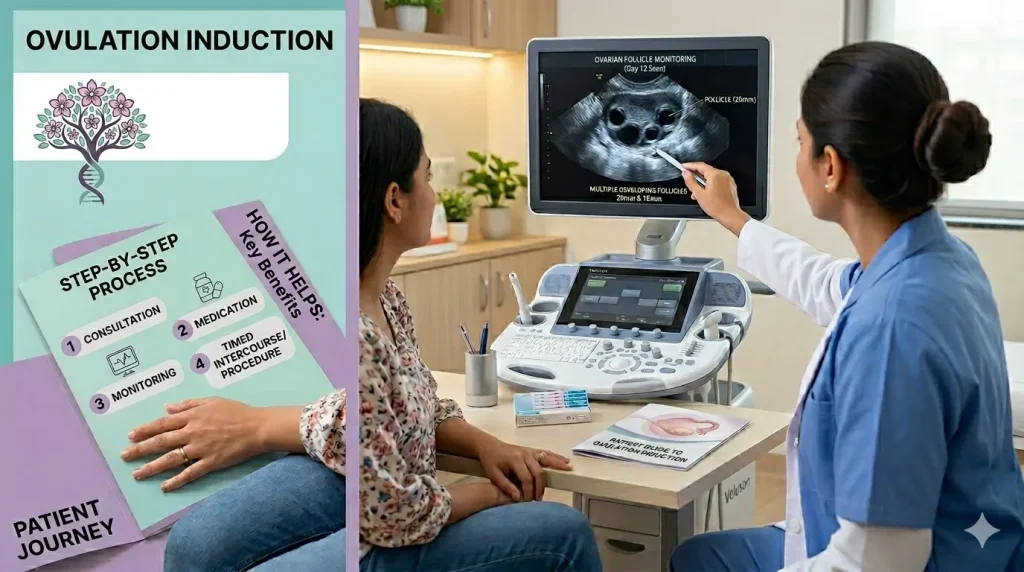
Follicle Monitoring: The Key to Successful Ovulation Induction
Medication alone isn’t enough. Ovulation induction must be monitored with transvaginal ultrasound to track how many follicles are growing and when they’re ready. Monitoring typically begins on Day 10-12 of the cycle and continues every 2-3 days until the dominant follicle reaches 18-20mm.
This monitoring serves two purposes. First, it tells the doctor the right time to give the HCG trigger injection, which causes final egg maturation and ovulation 36 hours later. Second, it allows cancellation of the cycle if too many follicles develop simultaneously, reducing the risk of multiple pregnancy.
For Pune’s IT professionals, the monitoring visits can usually be scheduled for early morning slots that don’t disrupt the work day. Most clinics in Kalyani Nagar, Hinjewadi and Baner offer pre-work appointment times for this reason.
Ovarian Hyperstimulation Syndrome (OHSS): What to Know
OHSS is the most significant risk of ovulation induction. The ovaries respond excessively to stimulation, becoming enlarged and leaking fluid into the abdomen. Mild OHSS is common and self-resolving. Moderate or severe OHSS (1-5% of cycles with gonadotropins) requires medical attention.
Risk factors for OHSS include PCOS, young age, low BMI and a high antral follicle count. To reduce risk, gonadotropin doses are kept low (2-4 follicles is the target, not 10-15 as in IVF). If too many follicles develop, the cycle is converted to IVF for safer egg retrieval or cancelled entirely.
Ovulation Induction in Pune: Local Context
Ovulation induction with follicle monitoring is one of the most commonly performed fertility procedures in Pune. Clinics in Kalyani Nagar, Wakad, Baner and Pimpri Chinchwad all offer this service. The low cost and minimal invasiveness make it the natural first step for young couples with anovulatory infertility.
Femcare Fertility in Kalyani Nagar, where Dr. Sayali Shitole Chavan practises, provides ovulation induction as part of a tailored fertility plan. For women with PCOS, Dr. Sayali’s approach includes metabolic assessment alongside the medication protocol, since insulin resistance significantly affects response to OI medications and is very common in the Pune population.
Frequently Asked Questions
Q: How many cycles of ovulation induction should I try?
Most guidelines recommend 3-4 cycles of ovulation induction before escalating to IUI or IVF. If ovulation occurs but pregnancy doesn’t result after 3 cycles, the next investigation step is usually a semen analysis review and possible IUI. If ovulation is not achieved despite medication, the protocol is adjusted.
Q: Does ovulation induction increase the risk of twins?
Yes, modestly. With oral agents like clomiphene or letrozole, the risk of twins is approximately 5-8%, compared to 1-2% in natural conception. With gonadotropin injections, the risk is higher if not carefully monitored. Careful follicle count monitoring and cycle cancellation when too many follicles develop reduces this risk significantly.
Q: Is ovulation induction painful?
The oral medications clomiphene and letrozole are tablets with minimal side effects. Some women experience mild hot flushes with clomiphene. Gonadotropin injections are given subcutaneously (under the skin) with a very fine needle and are usually well tolerated. Mild bloating as follicles grow is the most common complaint.
Q: Can I do ovulation induction at a regular gynaecology clinic in Pune?
Simple ovulation induction with oral medications can be managed at a well-equipped gynaecology clinic with ultrasound capability. Gonadotropin cycles with careful monitoring are best done at a dedicated fertility clinic. If IUI is combined with OI, an andrology lab for sperm preparation is needed.
Q: How do I know if ovulation induction is working?
Follicle monitoring scans show whether follicles are growing to the right size. An HCG injection triggers ovulation from a mature follicle. A progesterone blood test 7 days after the HCG trigger confirms ovulation occurred. A pregnancy test 14-16 days after the trigger confirms whether conception was successful.
Conclusion
Ovulation induction treatment in Pune is the simplest, most affordable entry point into fertility treatment. For women with PCOS or irregular cycles, it can be the difference between years of failed natural attempts and a successful pregnancy within a few months.
Dr. Sayali Shitole Chavan at Femcare Fertility, Kalyani Nagar, provides personalised ovulation induction protocols based on each patient’s hormonal profile, AMH and cycle history. Her PCOS-focused approach includes metabolic optimisation alongside medication, improving response and success rates.
Book a consultation at drsayalichavanivfdoctor to find out if ovulation induction is right for you.

Dr. Sayali Chavan - Shitole
Dr. Sayali Shitole Best IVF & Fertility Specialist in Pune is a reliable and among the Best IVF Clinic in Pune & IVF Centre in Pune. Dr. Sayali Shitole is equipped with all ultra-modern facilities IVF Clinic/IVF Centre and Test Tube Baby Centre in Pune.